Global launch of the Lancet-World Psychiatric Association Commission
The world is failing to tackle the persisting and increasingly serious global crisis of depression it is facing, according to a Lancet and World Psychiatric Association Commission on depression, which calls for a whole-of-society response to reducing the global burden of depression.
Despite abundant evidence that much can be done to prevent depression and aid recovery even in resource-limited settings, an estimated 5% of the adult population around the world in any year are living with depression [1]. In high-income countries, about half of people suffering from depression are not diagnosed or treated, and this rises to 80-90% in low- and middle-income countries. The COVID-19 pandemic has created additional challenges, with social isolation, bereavement, uncertainty, hardship, and limited access to healthcare taking a serious toll on the mental health of millions.
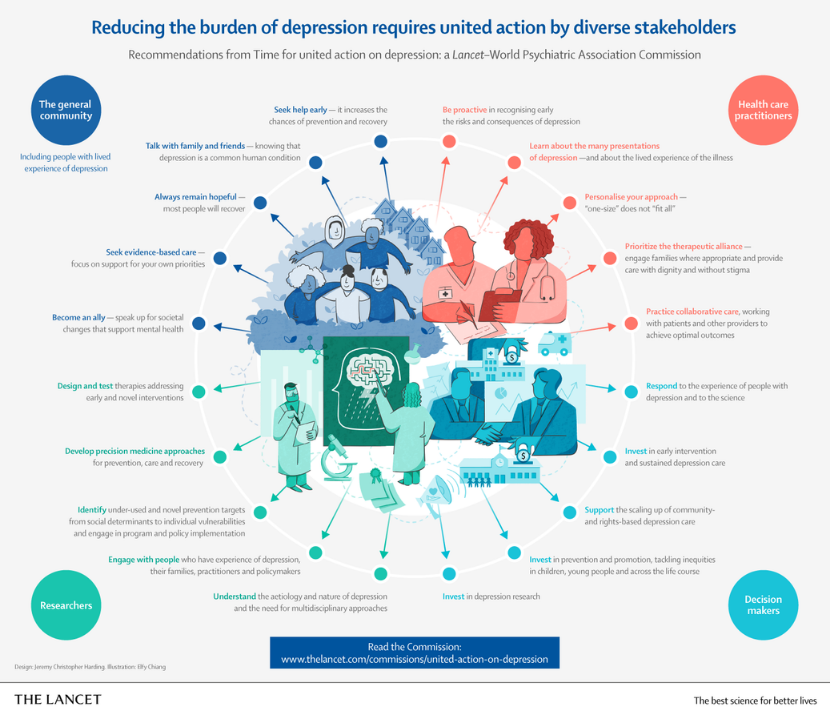
Against this background, the Commission ‘Time for united action on depression’ calls for concerted and collaborative efforts by governments, healthcare providers, researchers, people living with depression, and their families to improve care and prevention, fill knowledge gaps, and increase awareness to tackle one of the leading causes of avoidable suffering and premature death worldwide. It is authored by 25 experts from 11 countries spanning disciplines from neuroscience to global health and advised by people with experience of depression.
“Depression is a global health crisis that demands responses at multiple levels. This Commission offers an important opportunity for united action to transform approaches to mental health care and prevention globally. Investing in reducing the burden of depression will give millions of people the chance to become healthier, happier and more productive members of society, help to strengthen national economies, and advance the United Nation’s Sustainable Development Goals for 2030”, says Commission Chair Professor Helen Herrman from Orygen, National Centre for Excellence in Youth Mental Health and The University of Melbourne, Australia. [2]
Co-author Dr Charles Reynolds from the University of Pittsburgh, USA says, “We know that most individuals with depression at all stages of life will recover if they obtain adequate support and treatment. With sound science, political will, and shared responsibility, depression can be prevented and treated and potentially disabling consequences avoided. We must empower people with experience of depression together with families, practitioners, policymakers and civil society to address the tsunami of unmet need—through sharing their experiences to reduce stigma, supporting others with information about the condition and possibilities for help, and advocating for greater resources for evidence-based approaches.” [2]
A poorly recognised and understood condition
Depression is a common condition worldwide, yet despite this, many myths continue to surround it, perpetuating inaction. These include common misconceptions that depression is simply sadness, a sign of weakness, or restricted to certain cultural groups. The Commissioners stress that depression is a distinct health condition characterised by its persistence, substantial effect on daily functioning, and long-term health consequences. It can affect anyone, regardless of gender, background, social class, or age, there is variability in types and prevalence of depressive symptoms and signs among cultures and populations. The risk of depression rises in settings of adversity including poverty, violence, displacement and gender, racial and other forms of discrimination.
Depression is linked to a wide variety of chronic physical illnesses, and a person’s physical health can influence their mental health, and vice versa. At its worst, depression can lead to suicide. Studies indicate that 70%-80% of people who die by suicide in high-income countries, and around half of those in low- and middle-income countries, suffer from mental illness, of which depression is the most common cause. Depression also has an enormous, under-recognised social and economic toll on individuals, families, communities, and countries. Even before the COVID-19 pandemic, the loss in economic productivity linked to depression cost the global economy an estimated US$1 trillion a year [3].
“There is arguably no other health condition which is as common, as burdensome, as universal, or as treatable as depression, yet it receives little policy attention and resources”, says Commission Co- Chair Associate Professor Christian Kieling from the Universidade Federal do Rio Grande do Sul in Brazil. “Effective psychosocial and medical treatments are difficult to access, while high levels of stigma still prevent many people, including the high proportion of adolescents and young people at risk for or experiencing depression, from seeking the help required to have healthy and productive lives.” [2]
Prevention is essential to reducing the burden of depression
The Commission stresses the need for whole-of-society strategies that reduce exposure to both adverse experiences in childhood (including neglect and trauma) and across the lifespan to lower the prevalence of depression. Interventions are also needed at the individual level, focusing on lifestyle factors (eg, smoking, alcohol consumption, physical inactivity) and other risk factors such as intimate partner violence and stressful life events such as bereavement or financial crisis.
“Prevention is the most neglected aspect of depression. This in part because most interventions are outside of the health sector”, says co-author Dr Lakshmi Vijayakumar from SNEHA, Suicide Prevention Centre and Voluntary Health Services, Chennai, India. “In the face of the lifelong effects of adolescent depression, from difficulty in school and future relationships to risk of substance abuse, self-harm, and suicide, investing in depression prevention is excellent value for money. It is crucial that we put into practice evidence-based interventions that support parenting, reduce violence in the family, and bullying at school, as well promoting mental health at work and addressing loneliness in older adults. Common risk factors and high rates of depression among people with chronic health problems also support shared preventive approaches.” [2]
A personalised, staged approach to care
The Commissioners stress that the current system of classifying people with symptoms of depression into just two categories—either they have clinical depression or not—is too simplistic. They argue that depression is a complex condition with a diversity of signs and symptoms, severity levels, and duration across cultures and the life course.
The Commission supports a personalised, staged approach to depression care that recognises the chronology and intensity of symptoms and recommends interventions tailored to the specific needs of the individual and severity of the condition, ranging from self-help and lifestyle changes to psychological therapies and antidepressants to more intensive and specialised treatments such as electroconvulsive therary (ECT) for severe, refractory forms of the illness.
“No two individuals share the exact life story and constitution, which ultimately leads to a unique experience of depression and different needs for help, support, and treatment”, explains Commission Co-Chair Professor Vikram Patel from Harvard Medical School in the USA. “Similar to cancer care, the staged approach looks at depression along a continuum—from wellness, to
temporary distress, to an actual depressive disorder—and provides a framework for recommending proportional interventions from the earliest point in the illness.” [2]
At the same time, the Commission proposes that collaborative care strategies are adopted to scale up evidence-based interventions in routine care. They argue that using locally recruited, widely available and low-cost non-specialists such as community health workers and lay counsellors, not only addresses the acute shortage of skilled providers and financial barriers, but will also help reduce stigma and cultural barriers, while providing holistic care to patients and their families. While this is most important in low-income countries it is also relevant and useful universally as nowhere in the world is depression care adequate.
Ultimately, greater investment is needed to ensure that people receive the care they need where and when they need it, and the Commission underscores the importance of whole-of-government actions to reduce the damaging effects of poverty, gender inequity, and other social inequities on mental health. “Policies that reduce racial or ethnic inequities, systematic disadvantages experienced by women and support the fair distribution of income through universal health coverage and expanding opportunities for educational attainment can be potentially powerful preventive strategies”, says Herrman. “Tackling the climate emergency, the COVID-19 pandemic and other global and regional emergencies that exacerbate existing inequities and threats to health, including pursuit of the UN Sustainable Development Goals, must also be vital parts of efforts to
prevent depression.”[2]