STRASSER, Prof Roger
Australia - Founding Chair, Rural WONCA

Photo: Professor Roger Strasser receives his Rural WONCA Fellowship from Chair Dr Pratyush Kumar at the Rural WONCA Assembly in Wellington.
At the Rural WONCA Assembly in Wellington, Aotearoa New Zealand, the first ever Rural WONCA Fellowships were awarded to the five past chairs of the WONCA Working Party on Rural Practice. Among them was Professor Roger Strasser, the founding chair, who led the group from 1992 to 2004 and helped bring it into being at the WONCA World Conference in Vancouver that year.
Presented by current Chair Dr Pratyush Kumar, the fellowships honoured more than three decades of leadership, service and vision. We spoke with Professor Strasser during the conference to talk about the movement's beginnings, how rural practice has changed, and where he sees it going.
You were there at the start. How did the Working Party come about?
In 1992 I attended the WONCA World Conference in Vancouver. I had just been appointed as the first professor of rural health in Australia, and there were a lot of rural practitioners at that meeting with real energy about them. I connected with a rural doctor from South Africa, realised there were many of us in the same position, and called an ad hoc lunchtime meeting. Around 70 doctors from around the world came together, and that was the beginning of the Working Party on Rural Practice, which WONCA recognised that same year.
What struck us was how much we had in common. There were obvious differences between our countries, our systems and our contexts, but there was a genuine sense of shared experience and shared purpose. Out of that came a clear recognition: when you are talking about rural health, access is the issue, everywhere. Resources concentrate in the cities, distances and communications are always a challenge, and there is never enough health workforce. That is true of rural health right around the world.
The first World Rural Health Conference followed in China in 1996. Thirty years on, how has the movement changed?
That first conference was actually called the International Conference on Rural Medicine. We have moved a long way beyond a focus on medicine alone. Rural practice, rural generalism, is about all of the health professions working together as a team. This is the 21st of these conferences, and here in Wellington we have something like 950 participants from more than 36 countries. The sense of excitement and camaraderie is exactly what it was three decades ago, but the scope is far wider.

Photo: At the third conference in Sarawak in 1999, (from L to R) Dr John Wynn-Jones (Wales), the late Dr MK Rajakumar (host organiser, Malaysia), Dr Roger Strasser (Chair, WWPRP, Australia), Dr Jim Rourke (Canada), the late Dr John McLeod (Scotland).
You have advocated for rural health through decades of technological change. How do you see technology's role?
Technology has been part of this from the beginning, and in a very practical way. In 1987, two developments gave the rural health movement in Australia its foundation. The first was the audio teleconference, which let rural practitioners stay in their own communities and their own practices while still connecting and working together as a group. The second was the fax machine, which meant we could develop documents between us. That is how the Working Party did something unusual for its time. Rather than meeting only in person, we held audio conferences between conferences and drafted policy together, so that by the WONCA conference in Hong Kong in 1995 we could present a draft policy on training for rural practice. At the first world rural conference in China, two colleagues came to demonstrate this newfangled thing called the internet. They brought it on discs, because they could not be sure a telephone line out of the venue would connect to anything.
The upside has grown over time. In Australia, the first satellite continuing education for remote practitioners came through satellite television. Given the national passion for sport, the dishes were often in pubs, so the broadcasts went out on a Sunday morning and practitioners had to go to the pub to watch. It probably caused some conversation in the community about what the doctor, the nurse and the pharmacist were doing at the pub on a Sunday morning. Today it is very different. In British Columbia in Canada, for example, there is a real-time virtual support system where hospital specialists make themselves available, essentially on call, to a rural nurse, community health worker or doctor who needs them. That kind of support is possible now with the internet, and it is exciting to see the potential to keep people cared for in their own home, family and community.
But there are minuses too. The one we warned about in our policy, first developed in 1997, is this: technological enthusiasts go to policymakers and governments and promote computers and communication technology as a substitute for having real people providing care in rural and remote communities. That is the danger. Technology should support rural practitioners who are there and who stay. It cannot replace them.

Photo: Professor Strasser (centre) speaking at the Rural WONCA Council meeting in Wellington.
A theme across this conference has been that rural doctors tend not to wait for permission. Where does that ethos come from?
Necessity is the mother of invention. There are never enough rural health workforce to meet the need, and by and large rural practitioners live in the communities they serve. They are acutely aware of what their community needs, which means they tend to work together in teams. There is a lot of talk about teamwork in the cities and the big hospitals, but in my experience it happens more commonly in rural communities. It is about answering people's desire to stay in their community and be looked after there.
That requires being creative and being willing to take risks. One of the really exciting developments of the last decade is research describing what we now call clinical courage: rural practitioners being prepared to go beyond their initial comfort zone, often with distance support, to be there and stay there so the people in their community have the best possible care and wellbeing.
You have just been named among the first Rural WONCA Fellows, and this conference also saw the launch of GRACE. What do these moments signify?
The fellowship was completely unexpected, and very special. I see it as recognition that Rural WONCA is moving into a new stage, a new era. To be in a position, as a collective, to award fellowships supported by WONCA is exciting, and humbling to be among the first to receive one.
Just before the conference we also had the official launch of GRACE, the Global Rural Health Action, Collaboration and Excellence initiative. GRACE is about all the players in the rural health ecosystem, including remote and indigenous communities, working together, learning from one another, and taking what works in one place and putting it into practice in another. The action word matters. It is another sign that we are moving towards an exciting future for rural health, for rural practice, and for the wider WONCA family.
Looking back over three or four decades, what would you leave people with?
I often hear people say nothing has changed. Look at the headlines from ten, twenty, thirty years ago: not enough rural health practitioners of any kind, recruitment and retention a constant challenge. The headlines are the same, but the reality is quite different. The whole world has changed, and we have learned an enormous amount. There has been substantial, genuinely impactful research and experience. We are ready to act.
The other thing I would say is this. Meaningful improvements that really stick, that make a real difference to the health of people in rural and remote communities, come from thinking, planning and acting in decades, not years. This is about longevity. You have to deal with the immediate pressures in the here and now, of course, but you always take the long view. You recognise what is important, not only what seems urgent, and you keep building towards a better future for everyone.
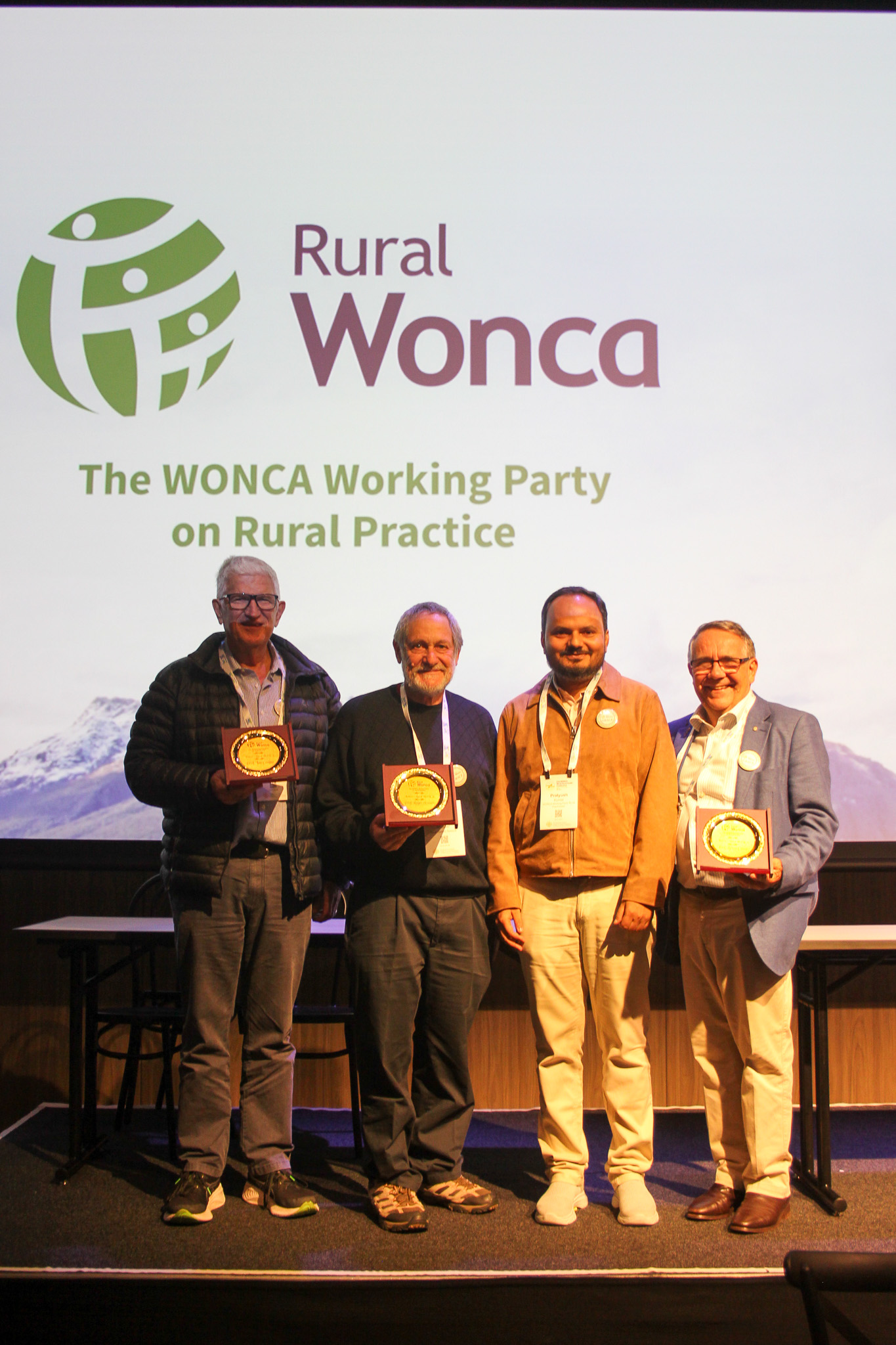
Photo: The inaugural Rural WONCA Fellowships were presented at the Rural WONCA Assembly in Wellington by Chair Dr Pratyush Kumar. Pictured (from L to R): Professor Ian Couper (South Africa, Chair 2007 to 2013), Professor Roger Strasser (Australia, Chair 1992 to 2004), Dr Pratyush Kumar (current Chair), and Professor Bruce Chater (Australia, Chair 2019 to 2025).
The inaugural Rural WONCA Fellows are:
- Professor Roger Strasser, Australia, Chair 1992 to 2004
- Professor Jim Rourke, Canada, Chair 2004 to 2007
- Professor Ian Couper, South Africa, Chair 2007 to 2013
- Dr John Wynn-Jones, Wales, UK, Chair 2013 to 2019
- Professor Bruce Chater, Australia, Chair 2019 to 2025
Professor Jim Rourke and Dr John Wynn-Jones were not present in Wellington, but they were warmly acknowledged as part of this first group of fellows.
Read the recap of the 21st World Rural Health Conference in Wellington
Read a history of the WONCA Working Party on Rural Practice